

- CDC
- Heart Failure
- Cardiovascular Clinical Consult
- Adult Immunization
- Hepatic Disease
- Rare Disorders
- Pediatric Immunization
- Implementing The Topcon Ocular Telehealth Platform
- Weight Management
- Monkeypox
- Guidelines
- Men's Health
- Psychiatry
- Allergy
- Nutrition
- Women's Health
- Cardiology
- Substance Use
- Pediatrics
- Kidney Disease
- Genetics
- Complimentary & Alternative Medicine
- Dermatology
- Endocrinology
- Oral Medicine
- Otorhinolaryngologic Diseases
- Pain
- Gastrointestinal Disorders
- Geriatrics
- Infection
- Musculoskeletal Disorders
- Obesity
- Rheumatology
- Technology
- Cancer
- Nephrology
- Anemia
- Neurology
- Pulmonology
Final USPSTF Recommendation on Breast Cancer Screening Lowers Starting Age from 50 to 40 Years, Highlights Racial Disparities
The USPSTF decision to reduce age of initiation is based on increasing rates of breast cancer in younger women; the group vows more research on higher mortality for Black women.
The United States Preventive Services Task Force (USPSTF) announced on April 30 a final recommendation statement on screening for breast cancer, lowering the age for initiation of screening mammography for women at average risk from age 50 to age 40 years and recommending ongoing surveillance every other year through age 74 years.1


©okrasiuk/stock.adobe.com
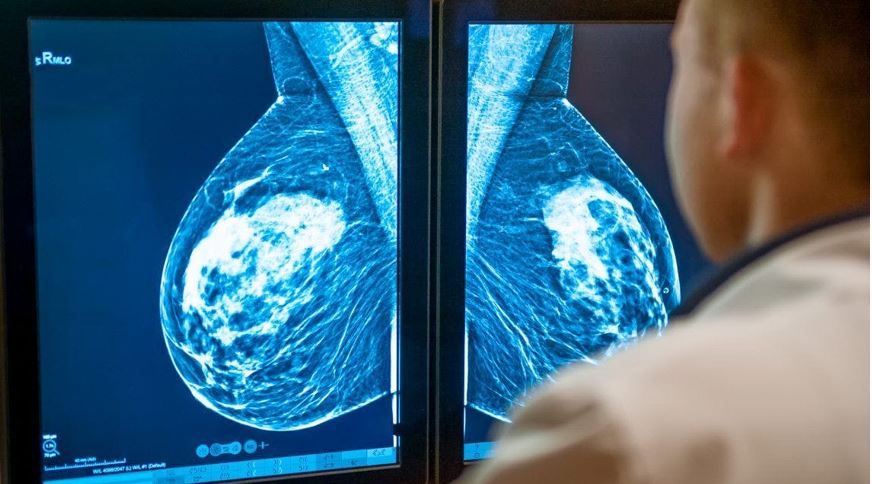
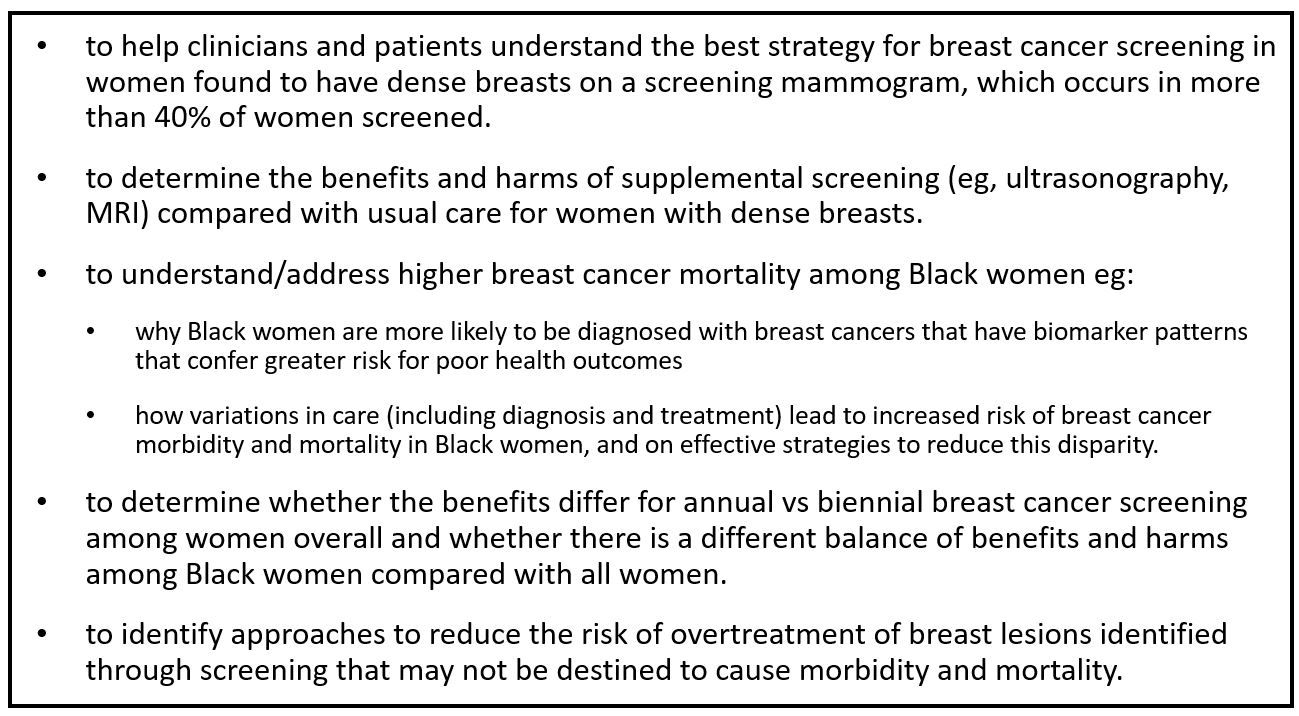
The statement indicates that there is not enough high-quality evidence to provide screening recommendations for women aged 75 years and older nor to assess the balance of benefits and harms of supplemental screening (eg, ultrasound) for women with dense breasts.1
The final statement, the first update since the organization’s 2016 recommendations, differs significantly from the previous iteration which recommended that women aged 40 to 49 years make an individual decision about when to commence screening based on their health history, preferences, and consultation with a health care professional.1
Changes in prevalence of breast cancer have played a role in the evolution of the Task Force recommendations. The rates of breast cancer for women in their 40s increased gradually between 2000 and 2015 but have risen more noticeably since then, increasing by approximately 2% per year, according to the USTSPF.2 “By starting to screen all women at age 40, we can save nearly 20 percent more lives from breast cancer overall," Task Force chair Wanda Nicholson, MD, MPH, MBA, said in the USPSTF announcement.2 "This new approach has even greater potential benefit for Black women, who are much more likely to die of breast cancer.”2
Raes of breast cancer for women in their forties increased gradually between 2000 and 2015 but have risen more noticeably since then, increasing by approximately 2% per year.
_________________________________________
Black women are 40% more likely to die of breast cancer than White women. Despite having a similar or even higher self-reported rate of mammography screening, they are more likely to be diagnosed with advanced stage cancer than other racial and ethnic groups and with more aggressive types of disease than White women. Diagnoses also are made at younger ages in Black women than among other racial/ethnic groups.
_________________________________________
Black women are 40% more likely to die of breast cancer than White women. Despite having a similar or even higher self-reported rate of mammography screening, they are more likely to be diagnosed with advanced stage cancer than other racial and ethnic groups and with more aggressive types of disease than White women. Diagnoses also are made at younger ages in Black women than among other racial/ethnic groups.
In fact, Black women are 40% more likely to die of breast cancer than White women.1 Despite having a similar or even higher self-reported rate of mammography screening, they are more likely to be diagnosed with advanced stage cancer than other racial and ethnic groups and with more aggressive types of disease than White women. Diagnoses also are made at younger ages in Black women than among other racial/ethnic groups.1
USPSTF modeling for the final statement estimated that the benefits of breast cancer screening for Black women are similar for the reduction of breast-cancer-related mortality but greater for life-years gained than for all women.1 While agreeing that a campaign to encourage screening initiation at age 40 years for Black women will likely help improve outcomes, the USPSTF acknowledged that even as an important first step, it is insufficient to “improve existing inequities,” the group wrote.2 “The USPSTF also agrees that improvements across the entire spectrum of breast cancer care are needed to reduce mortality for individuals experiencing disparities associated with lower breast cancer survival,” including follow-up evaluation and treatment.1
The decision to recommend screening every other year instead of every year was based on multiple factors. The Task Force used modeling data to compare benefits and harms between annual screening and biannual screening and found a more favorable trade-off of benefits and harms (eg, life-years gained, mortality averted per false-positive result) for the latter than the former.1
The update recommendations are based on results of a systematic literature review of studies that compared breast cancer screening strategies published in MEDLINE and the Cochrane Library through August 2022. Literature surveillance continued through March 2024. The main outcome measures reviewed were morbidity, mortality, progression to advanced cancers, and screening harms.3
Much more work ahead
The Task Force includes a list of research needs and gaps in screening for breast cancer that includes research1:


In an editorial accompanying the recommendation statement,4 Joann G. Elmore, MD, MPH, of the David Geffen School of Medicine at UCLA, and Christoph I. Lee, MD, MS, of the Fred Hutchinson Cancer Center and the University of Washington School of Medicine, echo the Task Force's own call for more comprehensive research into significant inequities in breast cancer mortality but also point to a trend that has been overlooked, "...the pressing issues of emerging use of artificial intelligence (AI) support tools for image interpretation."4 Taining and testing of these tools has been largely on older White women, Elmore and Lee wrote, which could continue to continue and exacerbate current disparities unless the research population is diversified.
"Overall, the updated USPSTF recommendations highlight a rapidly evolving intersection of technology and equity within an already complex health care ecosystem in which disparities remain a persistent problem...Moving ahead, population-level data collection throughout the entire breast care continuum is imperative to pinpoint interventions at individual, neighborhood, and health care facility levels that can help address existing disparities gaps across the entire screening and diagnostic episode of care.
"Until that is fully realized, clinicians must continue to do their best with the current resources, knowledge, and recommendations to ensure that enhancements in cancer outcomes benefit all individuals equitably," the concluded.






