- CDC
- Heart Failure
- Cardiovascular Clinical Consult
- Adult Immunization
- Hepatic Disease
- Rare Disorders
- Pediatric Immunization
- Implementing The Topcon Ocular Telehealth Platform
- Weight Management
- Monkeypox
- Guidelines
- Men's Health
- Psychiatry
- Allergy
- Nutrition
- Women's Health
- Cardiology
- Substance Use
- Pediatrics
- Kidney Disease
- Genetics
- Complimentary & Alternative Medicine
- Dermatology
- Endocrinology
- Oral Medicine
- Otorhinolaryngologic Diseases
- Pain
- Gastrointestinal Disorders
- Geriatrics
- Infection
- Musculoskeletal Disorders
- Obesity
- Rheumatology
- Technology
- Cancer
- Nephrology
- Anemia
- Neurology
- Pulmonology
HIV-Associated Intestinal Spirochetosis
A 33-year-old, sexually active homosexual HIV-positive man, with a CD4+ T-lymphocyte count of 258/µL and HIV-1 RNA level of 7079 copies/mL, presented to his primary care physician with left upper quadrant pain, urgency to defecate, and non-bloody watery diarrhea.
A 33-year-old, sexually active homosexual HIV-positive man, with a CD4+ T-lymphocyte count of 258/µL and HIV-1 RNA level of 7079 copies/mL, presented to his primary care physician with left upper quadrant pain, urgency to defecate, and non-bloody watery diarrhea. These signs and symptoms had been ongoing but subclinical for several years until they began to interfere with the patient's work as a massage therapist (eg, frequent bathroom visits throughout the day). His medical history was significant for GI infection with Blastocystis hominis and with Entamoeba coli, both of which resolved after treatment with iodoquinal and metronidazole, respectively. He had undergone laser excision of anal and perianal condylomata.
Four years after the resolved parasitic infections, the patient still experienced episodic, yet chronic, watery loose stools, and a discussion between the patient and a clinician resulted in further laboratory testing (stool culture) and imaging (colonoscopy). Stool cultures were negative for ova and parasites, and colonoscopy revealed grossly unremarkable mucosa. Biopsy specimens taken from the terminal ileum, right and descending colon, and rectum revealed minimal inflammation and architecturally intact crypts on histological evaluation. However, the colorectal mucosal biopsy specimens revealed a thin, "fuzzy" basophilic coating adhered to the luminal surface (Figure 1). Using a silver stain, numerous slender microorganisms, consistent with intestinal spirochetes, were present (Figure 2) and correlated with the thin hematoxiphilic luminal layer seen on the colonic biopsy specimens. Confirmatory polymerase chain reaction (PCR) was not performed.


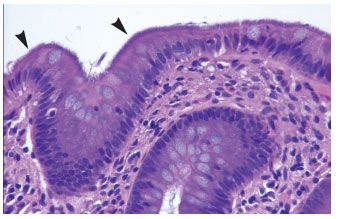
Figure 1.Biopsy specimen from right colon showing the luminal surface of the mucosa carpeted with a fine basophilic haze of spirochetes (hematoxylin-eosin stain, original magnification x400).


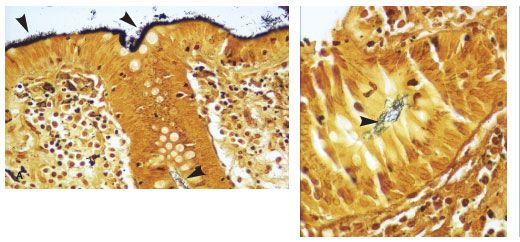
Figure 2. Biopsy specimen from colon at 55 cm demonstrated numerous slender organisms (left) (Steiner stain, original magnification x400). Individual crypt with readily recognizable spirochetes (right) (Steiner stain, original magnification x600).
Intestinal spirochetosis was first described in 10 symptomatic patients in 1967 by Harland and Lee.1Brachyspira aalborgi and Brachyspira pilosicoli are the most common organisms isolated, and the mode of transmission is generally unclear. Human intestinal spirochete populations are not related to nonintestinal spirochetes (eg, Treponema pallidum).2 Intestinal spirochete colonization has been compared with Helicobacter pylori infection in that initially, the patient may be symptomatic, but ultimately, the patient becomes an asymptomatic carrier.3 However, in cases of immunosuppression, these colonizers are thought to become opportunistic, and intestinal spirochetosis has been associated with appendicitis, abdominal pain, and rectal bleeding.4,5 Invasive and disseminated disease is extremely rare6 but has been reported in patients with HIV/AIDS.7,8
Clinically, symptomatic patients with intestinal spirochetosis most commonly experience a protracted course of watery diarrhea, crampy abdominal pain, or both. Endoscopic findings are generally unremarkable, as in this case. Diagnosis is typically made on histological examination-the organisms are recognized as a blue haze sitting on the mucosal surface and are better visualized with a silver impregnation technique (ie, using Steiner or Warthin-Starry stain). Although not routinely used, the immunohistochemical stain that identifies the spirochete T pallidum cross-reacts with the spirochetes that cause intestinal spirochetosis.9 The Brachyspira species may also be identified by molecular techniques, such as PCR, that target ribosomal DNA on either fecal samples or paraffin-embedded tissue.2
Men who have sex with men (MSM), whether HIV-positive or -negative, are at high risk for being colonized and are likely to be symptomatic. This same population is mostly affected by the spirochete B pilosicoli, whereas other human infection is mostly caused by B aalborgi.8 Owing to the sexual practices of MSM, the rectal micro-environment is believed to be altered in such persons, and along with frequent antibiotic treatment, MSM may be at risk for colonization and infection not only with parasitic organisms but also with spirochetes.10 HIV-positive heterosexual men show comparable rates and causes of intestinal infections.8 In MSM, the presence of HIV infection does not add to the pathogenicity of intestinal spirochetes or to a higher risk of spirochetosis.8 While there are no formal recommendations for the prevention of transmission of intestinal spirochetosis, standard hand hygiene is prudent.
In a small series, treatment of the symptoms with a course of metronidazole or penicillin benzathine has been reported to be successful.11 In the present case, the patient was not offered treatment at the time by his primary provider, and 3 years after this presentation, he still suffers from chronic diarrhea. As of July 2007, his CD4+ T-lymphocyte count was 500/µL and HIV-1 RNA level was less than 75 copies/mL.
Acknowledgements: Clinical Investigator Training Program: Beth Israel Deaconess Medical Center–Harvard/MIT Health Sciences and Technology, in collaboration with Pfizer Inc and Merck & Co (to H.P.S.).
References:
References1. Harland WA, Lee FD. Intestinal spirochaetosis. Br Med J. 1967;3:718-719.
2. Nodit L, Parizhskaya M. Intestinal spirochetosis. Arch Pathol Lab Med. 2004;128:823-824.
3. Abrams GD. Infectious disorders of the intestines. In: Ming SC, Goldman H, eds. Pathology of the Gastrointestinal Tract. 2nd ed. Baltimore: Williams & Wilkins; 1998:664.
4. Lindboe CF, Tostrup NE, Nersund R, Rekkavik G. Human intestinal spirochaetosis in mid-Norway. A retrospective histopathological study with clinical correlations. APMIS. 1993;101:858-864.
5. Henrik-Nielsen R, Lundbeck FA, Teglbjaerg P, et al. Intestinal spirochetosis of the vermiform appendix. Gastroenterology. 1985;88:971-977.
6. Shah RN, Stosor V, Badve S. Pathologic quiz case. Colon biopsy in a patient with diarrheaâpossible etiologic agent. Arch Pathol Lab Med. 2001;125:699-700.
7. Kostman JR, Patel M, Catalano E, et al. Invasive colitis and hepatitis due to previously uncharacterized spirochetes in patients with advanced human immunodeficiency virus infection. Clin Infect Dis. 1995;21:1159-1165.
8. Körner M, Gebbers JO. Clinical significance of human intestinal spirochetosis-a morphologic approach. Infection. 2003;31:341-349.
9. Uhlemann ER, Fenoglio-Preiser C. Intestinal spirochetosis. Am J Surg Pathol. 2005;29:982.
10. Surawicz CM, Roberts PL, Rompalo A, et al. Intestinal spirochetosis in homosexual men. Am J Med. 1987;82(3 spec no):587-592.
11. Klinger ET, Bernal K, Paustian F, et al. A 48-year-old HIV-positive man with chronic intermittent diarrhea. Clin Infect Dis. 2004;39:1174, 1239-1240.
12. Esteve M, Salas A, Fernández-Bañares F, et al. Intestinal spirochetosis and chronic watery diarrhea: clinical and histological response to treatment and long-term follow up. J Gastroenterol Hepatol. 2006;21:1326-1333.